



























Calculous prostatitis is accompanied by increased urination, dull pain in the lower abdomen and perineum, erectile dysfunction, the presence of blood in the seminal and prostate fluid. Calculous prostatitis can be diagnosed using a digital examination of the prostate, ultrasound of the prostate gland, urography and laboratory examination. Conservative therapy for calculous prostatitis is carried out with the help of medications, herbal medicine and physiotherapy; If these measures are ineffective, stone destruction with low-intensity laser or surgical removal is indicated.
General information
Calculous prostatitis is a form of chronic prostatitis, associated with the formation of stones (prostatolites). Calculous prostatitis is the most common complication of a long-term inflammatory process in the prostate gland, which specialists in the field of urology and andrology have to deal with. During preventive ultrasound examination, prostate stones are detected in 8. 4% of men of various ages. The first age peak in the incidence of calculous prostatitis occurs at the age of 30-39 years and is due to the increase in cases of chronic prostatitis caused by STDs (chlamydia, trichomoniasis, gonorrhea, ureaplasmosis, mycoplasmosis, etc. ). In men 40-59 years old, calculous prostatitis, as a rule, develops against the background of prostate adenoma, and in patients over 60 years old it is associated with a decline in sexual function.

Causes of calculous prostatitis
Depending on the cause of formation, prostate stones can be true (primary) or false (secondary). Primary stones first form directly in the acini and ducts of the gland, secondary stones migrate to the prostate from the upper urinary tract (kidneys, bladder or urethra) if the patient has urolithiasis.
The development of calculous prostatitis is caused by congestive and inflammatory changes in the prostate gland. Impaired emptying of the prostate glands is caused by BPH, irregular or lack of sexual activity and a sedentary lifestyle. Against this background, the addition of a slow infection of the genitourinary tract leads to blockage of the prostate ducts and a change in the nature of the prostate secretion. On the other hand, prostate stones also support a chronic inflammatory process and stagnation of secretions in the prostate.
In addition to stagnation and inflammatory phenomena, an important role in the development of calculous prostatitis is played by urethro-prostatic reflux - the pathological reflux of a small amount of urine from the urethra into the prostate ducts during urination. At the same time, the salts contained in the urine crystallize, thicken and over time turn into stones. The causes of urethro-prostatic reflux can be strictures of the urethra, trauma of the urethra, atony of the prostate and seminal tuberculosis, previous transurethral resection of the prostate gland, etc.
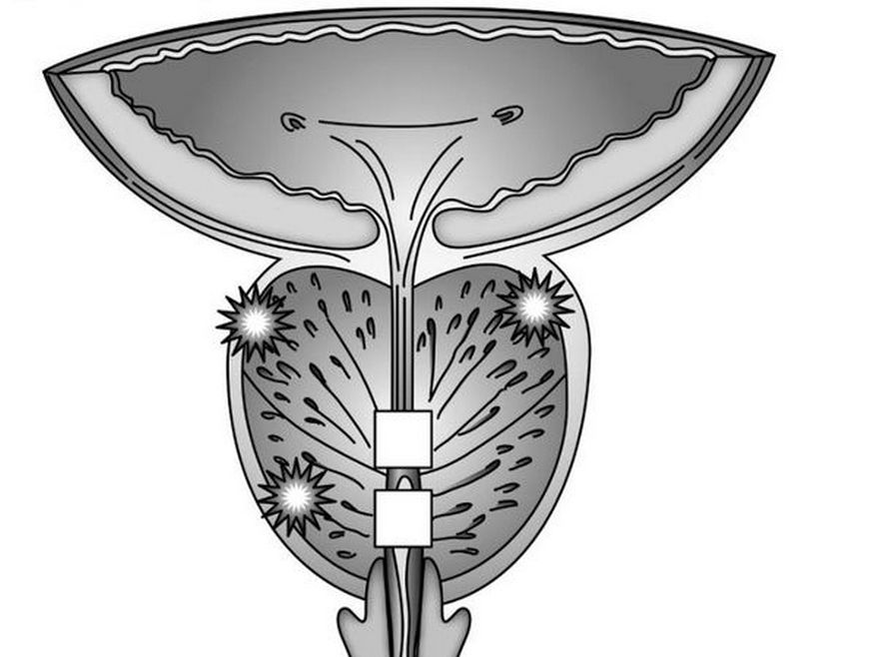
The morphological core for prostate stones are amyloid bodies and desquamated epithelium, which gradually "fill" with phosphate and lime salts. Prostate stones lie in cystically distended acini (lobules) or excretory ducts. Prostatoliths are yellow in color, spherical in shape and vary in size (on average from 2. 5 to 4 mm); can be single or multiple. In terms of their chemical composition, prostate stones are identical to bladder stones. With calculous prostatitis, oxalate, phosphate and urate stones are most often formed.
Symptoms of calculous prostatitis
Clinical manifestations of calculous prostatitis generally resemble the course of chronic inflammation of the prostate. The main symptom in the clinic of calculous prostatitis is pain. The pain is dull, aching in nature; located in the perineum, scrotum, on the pubis, sacrum or coccyx. Aggravation of painful attacks may be associated with defecation, sexual intercourse, physical activity, prolonged sitting on a hard surface, prolonged walking or bumpy driving. Calculous prostatitis is accompanied by frequent urination, sometimes with complete retention of urine; hematuria, prostatorrhea (flow of prostate secretions), hemospermia. It is characterized by decreased sexual desire, weak erection, impaired ejaculation and painful ejaculation.
Endogenous prostate stones can remain in the prostate gland for a long time without symptoms. However, a long course of chronic inflammation and associated calculous prostatitis can lead to the formation of a prostate abscess, the development of vesiculitis, atrophy and sclerosis of the glandular tissue.
Diagnosis of calculous prostatitis
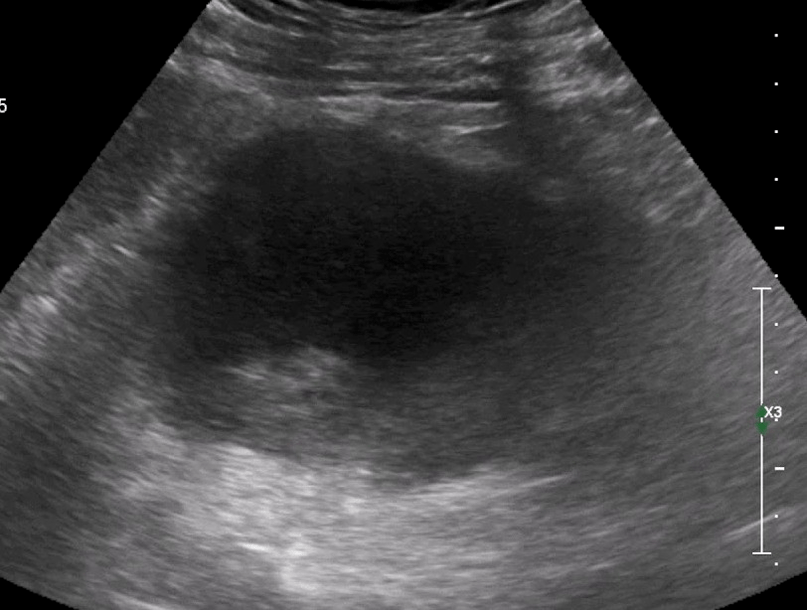
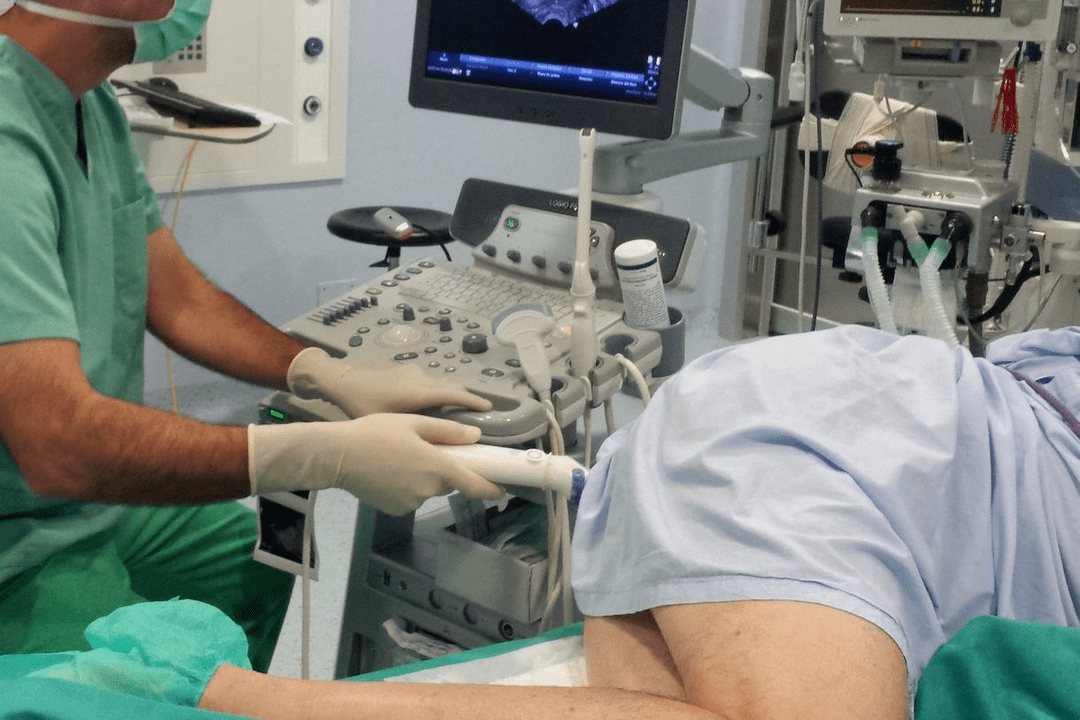
To establish a diagnosis of calculous prostatitis, a consultation with a urologist (andrologist), an assessment of existing complaints and a physical and instrumental examination of the patient is required. When performing a digital rectal examination of the prostate, the bumpy surface of the stones and a type of crepitus are determined by palpation. Using transrectal ultrasound of the prostate gland, stones are detected in the form of hyperechoic formations with a clear acoustic trace; their location, quantity, size and structure are clarified. Sometimes urography, CT and MRI of the prostate are used to detect prostatitis. Exogenous stones are diagnosed by pyelography, cystography and urethrography.
Instrumental examination of a patient with calculous prostate is complemented by laboratory diagnostics: examination of prostate secretions, bacteriological culture of secretions and urine from the urethra, PCR examination of scrapings for sexually transmitted infections, biochemical analysis of blood and urine, determination of prostate level. -specific antigen, sperm biochemistry, ejaculate culture, etc.
During examination, calculous prostatitis is distinguished from prostate adenoma, tuberculosis and prostate cancer, chronic bacterial and bacterial prostatitis. In calculous prostatitis not associated with prostate adenoma, the volume of the prostate gland and the PSA level remain normal.
Treatment of calculous prostatitis

Uncomplicated stones in combination with chronic inflammation of the prostate gland require conservative anti-inflammatory therapy. Treatment of calculous prostatitis includes antibiotic therapy, non-steroidal anti-inflammatory drugs, herbal medicine, physiotherapeutic procedures (magnetic therapy, ultrasound therapy, electrophoresis). In recent years, low-intensity lasers have been successfully used to noninvasively destroy prostate stones. Prostate massage for patients with calculous prostate is strictly contraindicated.
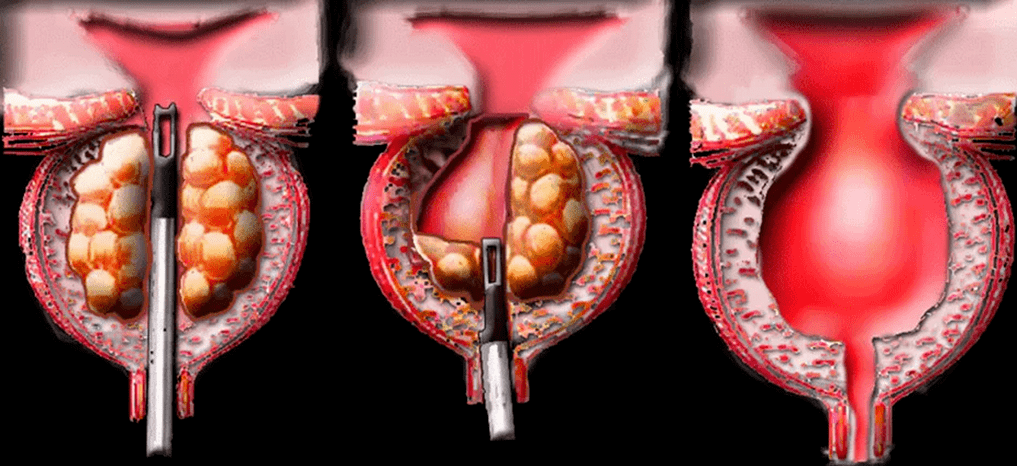
Surgical treatment of calculous prostatitis is usually required in the case of a complicated course of the disease, its combination with prostate adenoma. When an abscess of the prostate is created, the abscess opens and together with the discharge of pus, the passage of stones is also observed. Sometimes mobile exogenous stones can be instrumentally pushed into the bladder and subjected to lithotripsy. Removal of fixed stones of large size is carried out in the process of perineal or suprapubic section. When calculous prostatitis is combined with BPH, the optimal method of surgical treatment is adenomectomy, TUR of the prostate, prostatectomy.
Treatment of calculous prostatitis
Calculous prostatitis is an inflammation of the prostate gland, complicated by the formation of stones. This type of prostatitis is a consequence of long-term chronic inflammation of the prostate. The disease is accompanied by frequent urination, annoying pain in the lower abdomen and perineum, erectile dysfunction and the presence of blood inclusions in the ejaculate.
Causes of this disease
Calculous is a form of chronic prostatitis characterized by the formation of stones. The disease is often a complication of a long-term inflammatory process in the prostate. Against the background of chronic inflammation under the influence of negative internal and external factors, secretion stagnates, which over time crystallizes and turns into stones.
In addition to congestion and inflammatory phenomena, a major role in the development of calculous prostatitis is played by urethro-prostatic reflux, characterized by the pathological reflux of a small amount of urine from the urethra into the ducts of the prostate gland during urination. The salts contained in the urine gradually crystallize and over time turn into dense stones. Common causes of prostatic acid reflux:
- injuries of the urethra;
- atony of the prostate gland and seminal tuberculosis;
- previous surgical interventions and invasive procedures.
Other pathologies that increase the risk of prostate stone formation:
- varicose veins of the small pelvis;
- metabolic disorders due to systemic pathologies;
Factors that contribute to the development of calculous prostatitis:
- an inactive lifestyle that contributes to the development of stagnant processes in the pelvic organs;
- irregular sex life;
- alcohol abuse, smoking;
- uncontrolled use of certain groups of drugs;
- damage to the prostate during surgical procedures, long-term catheterization.
Types of stones in calculous prostatitis
According to the number of stones, single and multiple are distinguished. Depending on the underlying causes, prostate stones are:
- True. They are formed directly in the acini and ducts of the gland.
- Fake. They migrate to the prostate from the upper urinary tract: kidneys, bladder, urethra.
Stone formation in the prostate gland is identical in composition to bladder stones. With calculous prostatitis, the following types of stones are most often formed:
Symptoms of the disease
Symptoms of calculous prostatitis resemble the course of a chronic inflammatory process. The main symptom in the clinical picture of the disease is pain, the nature of which can be aching and dull. Pain localization: sacrum or coccyx.
A painful attack worsens during defecation, sexual intercourse, physical activity, prolonged standing on a hard surface and prolonged walking.
Other symptoms of pathology:
- frequent urination or complete retention of urine;
- hematuria and the presence of blood inclusions in the ejaculate;
- prostatorrhea – flow of prostate secretions;
- decreased sexual desire, erectile dysfunction, painful ejaculation;
- neurological disorders: nervousness, increased fatigue, insomnia.
If you have any of the above symptoms, you should make an appointment with a urologist as soon as possible. The lack of adequate treatment and the long course of chronic calculous prostatitis is fraught with serious, sometimes life-threatening consequences:
- atrophy and sclerosis of glandular tissue;
- prostate abscess.
Diagnosing
To make an accurate diagnosis, a consultation with a urologist-andrologist is necessary. During the initial examination, the specialist carefully listens to the patient's complaints, collects the anamnesis and asks additional questions that will help determine the causes of prostatitis and risk factors.
Next, the doctor performs a rectal examination of the prostate, which involves palpating the gland through the rectum. The technique allows you to assess the size, shape, structure of the gland, detect stones, determine the inflammatory process increasing in size and pain during pressure. To confirm the diagnosis, additional laboratory and instrumental methods are prescribed.
Laboratory diagnosis
A number of additional laboratory tests used to diagnose calculous prostatitis:
- Culture of prostate secretions. An important informative method for identifying pathogenic microorganisms and diagnosing the inflammatory process in the prostate gland.
- Urine culture. It allows you to detect a pathogenic infection in the urine, as well as determine its type and concentration. Culture is performed to clarify the diagnosis if inflammation of the prostate gland is suspected.
- PCR study of scrapings. It allows you to detect sexually transmitted infections and identify the pathogen.
- PSA analysis. It allows you to rule out prostate cancer, which often appears against the background of prostatitis.
- General clinical analysis of blood and urine. It is prescribed to identify hidden inflammatory processes in the urinary tract and kidney disorders.
- Spermogram. Ejaculate analysis to rule out or confirm infertility.
Instrumental diagnostics
Instrumental methods used to diagnose pathology:
Ultrasound of the prostate. It allows you to detect stones, clarify their location, quantity, size, structure. Ultrasound will also help distinguish inflammation of the prostate from other diseases associated with similar symptoms.
Survey of urography. A contrast-enhanced X-ray method that makes it possible to detect prostate stones, their size and location.
CT or MRI of the prostate. It allows layer-by-layer scanning of the prostate gland and surrounding tissue. Using CT or MRI images, the doctor can study the structure of the prostate in detail, detect pathological foci, evaluate their location, size and relationship with the surrounding tissue.
Treatment of calculous prostatitis
If the disease is uncomplicated and the general condition of the patient is satisfactory, the treatment of calculous prostatitis is carried out on an outpatient basis. If the disease is accompanied by complications, combined with prostate adenoma, hospitalization of the patient is required.
Conservative treatment
The main goals of conservative therapy are the elimination of pathological symptoms. For this, the patient is prescribed a course of drug therapy, which includes the use of the following groups of drugs:
- Antibiotics. Destroy the infection, stop the inflammation. The type of drug, the dose and the duration of the course for each patient are determined individually.
- Nonsteroidal anti-inflammatory drugs. They stop the inflammatory process and help eliminate pathological symptoms: pain, swelling.
- Antispasmodics. It relieves muscle spasms and relieves pain.
- Alpha adrenergic blockers. Facilitate the urination process.
- Vitamin-mineral complexes, immunomodulators. Strengthen the immune system and promote rapid healing.
As a complement to complex drug therapy, doctors often prescribe physiotherapeutic procedures that allow:
- elimination of stagnant processes;
- activate tissue regeneration.
- The most effective physiotherapy methods for calculous prostatitis:
- ultrasound therapy, shock wave therapy.
Effective treatment of calculous prostatitis is provided by lifestyle changes. In order to prevent relapses, it is recommended to include physical activity, especially if the work forces you to lead a sedentary lifestyle. Moderate physical activity improves blood circulation in the pelvic organs, eliminates congestion and strengthens local immunity.
Surgery
Surgical treatment is performed in case of complicated course of the disease and combination with prostate hyperplasia. When an abscess forms, the surgeon opens the abscess. Along with the discharge of pus, the passage of stones is often observed. Large fixed stones are removed during a perineal or suprapubic section. When calculous prostatitis is combined with benign prostatic hyperplasia, the optimal methods of surgical treatment are transurethral resection of the prostate.
Chronic calculous prostatitis
The term calculous prostate defines the pathology of the prostate gland, in which stones are formed in its tubules. This disease is characterized by impaired erection of the penis and pain in the groin area.
Causes and mechanism of development of calculous prostatitis
A prolonged inflammatory process or congestion in the prostate tubules leads to the accumulation of secretions and mucus in them. Bacteria settle in these accumulations and calcium salts precipitate. Over time, the mucus becomes denser and turns into small stones like sand. They stick together and form pebbles.
There are several predisposing factors for the development of calculous prostatitis:
- Chronic sexually transmitted infections (STDs)
- prolonged course of the infectious process with inflammation of the ducts and tissues of the prostate gland;
- prostate overload, which is mainly related to a man's irregular sex life;
- Urethro-prostatic reflux - pathological return of a small volume of urine into the prostate;
- genetic predisposition – the presence of relatives with calculous prostate.
Knowing the causes of the development of stones in the prostate gland is necessary for a qualitative and adequate etiological therapy, which helps prevent the redevelopment of calculous prostatitis.
Symptoms of calculous prostatitis
Symptoms of calculous prostatitis develop over a long period of time and a man may not pay attention to them. The clinical picture of the disease may include symptoms such as dull pain in the bottom of the abdomen and in the lower back, sacrum, perineum and pubis.
The pain may begin or intensify after defecation, sexual intercourse, intense physical activity and other provoking factors. Dysuric disorders are noted - frequent urge to go to the toilet, painful or difficult urination, burning in the urethra and at the bottom of the abdomen, and sometimes urinary retention occurs due to obstructions in the form of stones.
Patients experience prostatorrhea - involuntary secretion of the prostate gland during rest or during physical exertion, straining during bowel movements or urination. There may be blood in the urine and semen.
Almost always, against the background of continuous inflammation with the formation of stones, sexual dysfunctions develop - weakened erection, premature ejaculation, decreased libido.
The main signs of calculous prostatitis include:
- erectile dysfunction;
- pain in the groin area, which can be spasmodic and paroxysmal in nature;
- during ejaculation - indicates damage to the vessels of the prostate tubes from the sharp edges of the stones;
- premature and painful ejaculation.

Such symptoms lead to a decrease in sexual desire.
Often men attribute this to the age factor, mistakenly believing that such sexual dysfunctions will not disappear. Sometimes they begin to self-medicate using various erection-stimulating drugs (PDE-5 inhibitors).

This approach is very dangerous, as it can worsen the course of the pathological process and lead to the development of complications.
Prostatitis is a pathological inflammatory process in the prostate gland of a man. In most cases, it is caused by an infection, which gradually leads to a chronic, long-term course of the disease and the development of complications.
Treatment of calculous prostatitis is complex
- antibiotics,
- anti-inflammatory drugs,
- enzymes
- immunological drugs
- phytotherapy,
- physiotherapeutic procedures.
Antibacterial agentsprescribed as part of etiotropic treatment. Taking them is necessary to suppress the activity of the causative agent of the infectious-inflammatory process. This can be both non-specific microbial flora (streptococci, staphylococci, enterococci, Escherichia coli, Proteus), and specific pathogens of urogenital infections - gonococcus, chlamydia, ureaplasma, trichomonas, etc.
The choice of antibiotics can be based on the results of a culture study of prostate secretions and on determining the sensitivity of the microbial pathogen to the drugs. Sometimes antibiotics are prescribed empirically based on the scientifically proven antimicrobial effectiveness of the drugs. The selection of antibiotics, the determination of the dose and the duration of their use can be carried out exclusively by the attending physician, since their uncontrolled use can lead to serious complications and worsen the course of the underlying disease.
If the tissues of the prostate gland are parasitized by many associated microbial flora (bacterial, viral microorganisms, protozoa), the etiotropic therapy regimen will consist of a complex of different drugs that act on a certain antimicrobial spectrum.
To stimulate the immune defense of the bodyand its resistance to infections, immunomodulating drugs are prescribed - Immunomax, Panavir, Interferon and its derivatives. To improve the antimicrobial effect of etiotropic drugs, together with them, enzymatic agents are prescribed - longidase, chemotypsin. They facilitate the distribution of antibiotic active substances in the affected tissues, have an indirect analgesic effect and have an anti-inflammatory and regenerative effect.
The pain syndrome is relieved byusing non-steroidal anti-inflammatory drugs. Along with antibiotic therapy, probiotics are prescribed to prevent the development of intestinal dysbiosis. To protect the liver parenchyma from the toxic effects of antibacterial drugs and to improve its functional state, hepatoprotectors are prescribed. After alleviating acute inflammatory phenomena, physiotherapeutic procedures are prescribed - laser treatment, magnetic therapy, mud therapy, galvanization, medical electrophoresis, reflexogenic therapy, hardware treatment, etc.
This improves metabolic processes, microcirculation, lymphatic drainage and prostate tissue trophism, stimulates the return of its functional state and helps resolve inflammatory processes. A low frequency laser is used to destroy the stones. It crushes stones and allows small stones to pass out of the tubules. In case of complications in the form of prostate adenoma or abscess (a limited cavity filled with pus), surgical intervention is performed.
It involves removing part of the prostate gland (resection). To avoid this, at the first signs of pathology, expressed in erectile dysfunction, you should consult a doctor. Self-medication or ignoring the problem always leads to the subsequent development of complications.